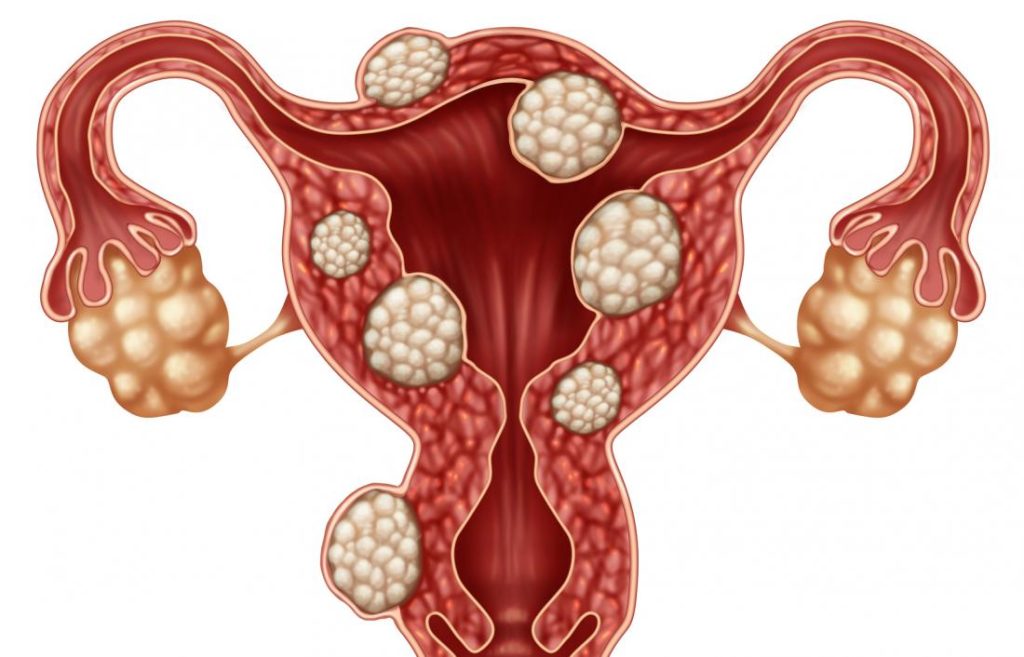
Myoma is the most common benign uterine tumor, it can be found in about 70% of women.
In our practice, we most often use FIGO classification, which reflects the location of the node in the body of the uterus:
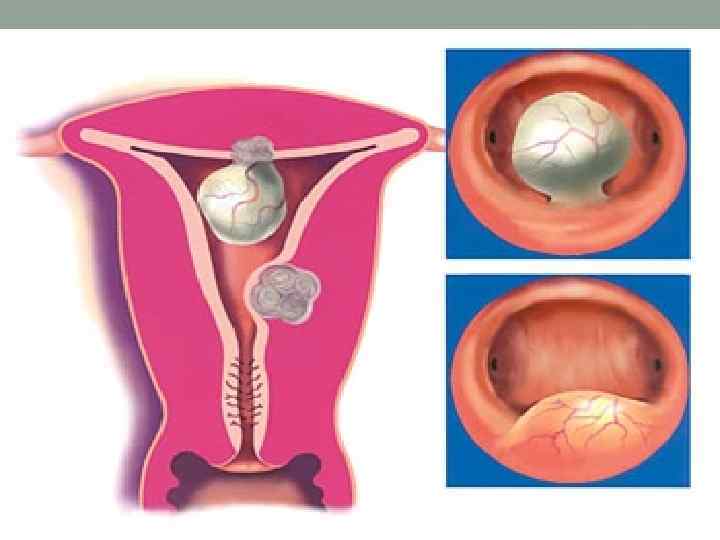
- Nodes of the type 0.1.2 are located in the uterine cavity (SumbMucous type 0) or partially in the cavity partially in the wall of the uterus (type 1 and 2)
- Type 3.4- are located in the thickness of the walls of the uterus (interstitial)
- Type 5.6 nodes- partially subsistent in the wall of the uterus (the serous membrane is the surface shell of the uterus)
- Type 7 -is completely located on the outside from the uterus, connects to it with a leg
- Type 8-sophomic location of the nodes-for example, in the cervix
In most cases, this pathology proceeds asymptomatic.
Manifestations more often depend on the location of the node and its size.
The most frequent symptoms of myoma:
- abundant and painful menstruation (characteristic more for the nodes located in the cavity and wall of the uterus), which leads to a decrease in hemoglobin
- acute pain in the lower abdomen- in case of violation of the node (usually with large nodes) or when the "birth" of the submucous node
- an increase in the volume of the abdomen (sometimes the body of the uterus with myomas can reach up to 20 and even 30 weeks of pregnancy)
- Infertility (if the nodes are located in the areas of the uterine mouths and interfere with the migration of spermatozoa or submucous and interfere with implantation of the fetal egg)
- compression and violation of the work of the surrounding organs- bladder (rapid urination), intestines (constipation)
Diagnostics:
- An annual examination of a gynecologist’s obstetrician, during which the patient’s complaints and bimanual manual examination are assessed
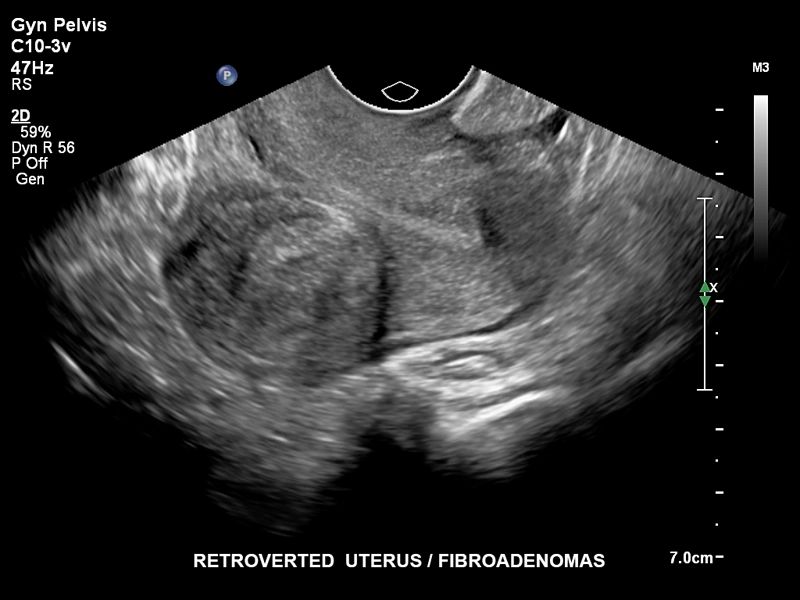
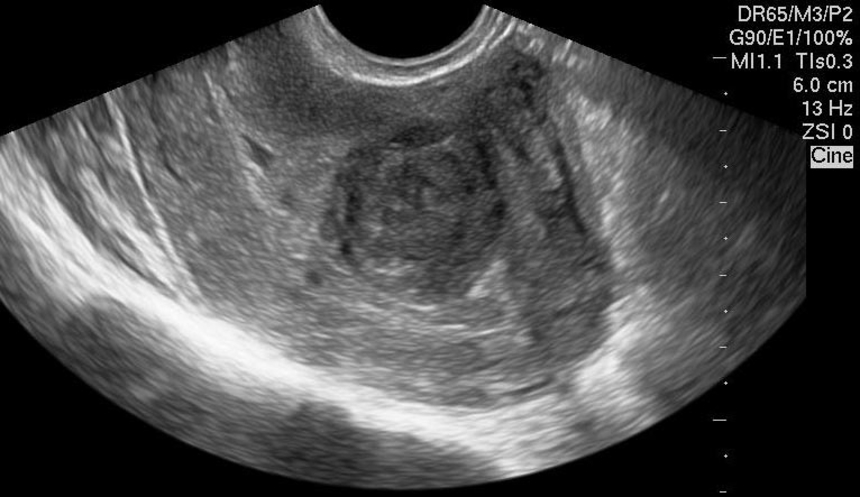
- Ultrasound of the pelvic organs - in modern realities, a very accessible and informative method in the diagnosis of myoma, evaluate their size and location. Today there is a method of an ultrasound of the pelvic organs with 3D reconstruction, which is more informative in terms of diagnosis of the type of submucous node (type 0, type 1, type 2)
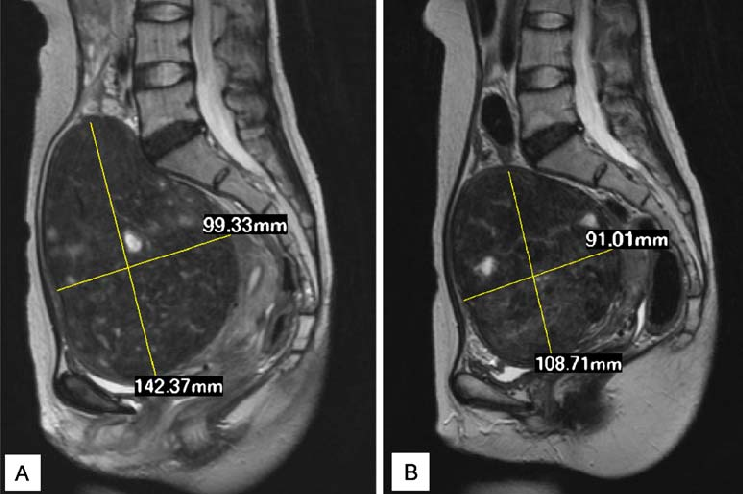
- In complex and incomprehensible cases, an MRI of the pelvic organs is used
- Hysteroscopy is a highly informative method in the diagnosis of endometrial pathology, including submucous myomatous nodes.
The treatment of myoma is quite difficult, since the exact causes of its occurrence are not clear. Accordingly, there is no single correct method. The choice of the method is determined, as a rule, with complaints (for example, constipation when the rectum is compressed), symptoms (abundant menstruation, anemia) fibroids and women reproductive plans.
With small sizes and asymptomatic course, a dynamic observation is very often enough- examination of the doctor and ultrasound of the OMT once every 6-12 months.
Largely can be divided by treatment methods into 2 large groups: medication and operational.
No drug method will force a myomatous node to disappear. The main task of this method is to reduce symptoms, most often it is abundant menstruation. The main groups of drugs:
- Hormone gonadotropin-rilying agonists (expensive drugs, put a woman into a menopause, the effect is used, more often used as preoperative preparation),
- The hormonal spiral “Mirana” (dosedly distinguishes hormones acting on the endometrium, which reduces the volume of menstrual bleeding. But it does not fit with deformation of the uterine cavity or with large uterine fibroids),
- Selective modulators of progesterone receptors (Esmia, the drug did not receive widespread use),
- COC (the main function of combined oral contraceptives is contraception, but in parallel these drugs reduce the volume of lost blood during menstruation).
Operational methods:
- The myomectomy is the renewal of the node with laparoscopic or laparotomic access, the submucous nodes are preferably removed using hysteroregectoscopy. These methods allow you to maintain fertility (the ability to give birth in the subsequent)
- Hysterectomy is a uterine dedication (often used in women performing reproductive function and with multiple uterine fibroids of large sizes)
- embolization of the uterine arteries (with single nodes that do not affect the uterine cavity; the method is limited by the size of the node - usually not more than 8 cm)
In the gynecological department of UZ 6 CGB, hysterosectoscopy of submucous nodes, removal of myomatous nodes with laparoscopic and laparotomic access, and uterine extirpation for fibroids are carried out.